Rehabilitative Exercise Reduced the Impact of Peripheral Artery Disease on Vascular Outcomes in Elderly Patients with Claudication: A Three-Year Single Center Retrospective Study

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
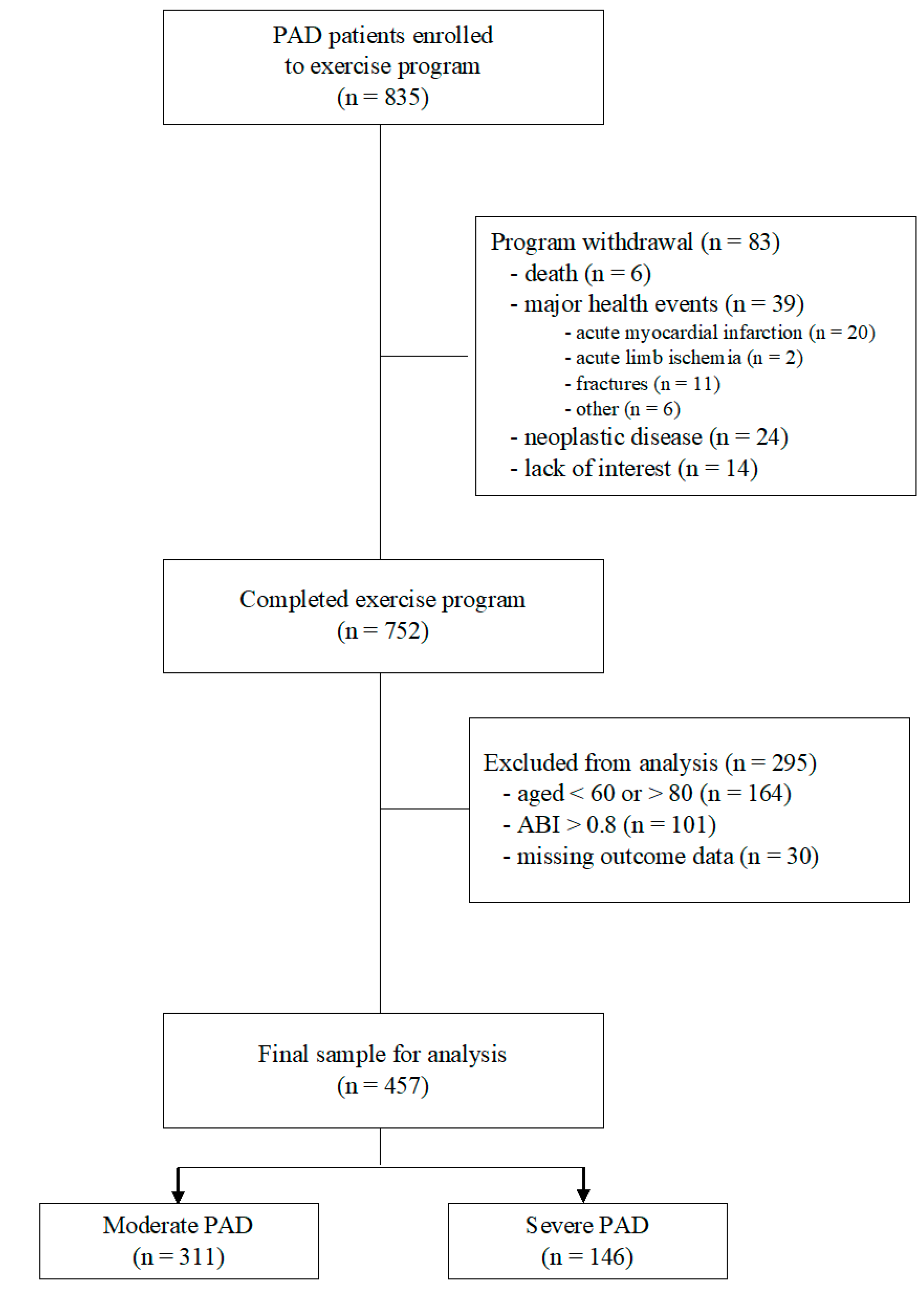
2.1. Study Population
2.2. Exercise Program
2.3. Outcomes
2.4. Study Variables
2.5. Statistical Analysis
3. Results
3.1. Exercise Program
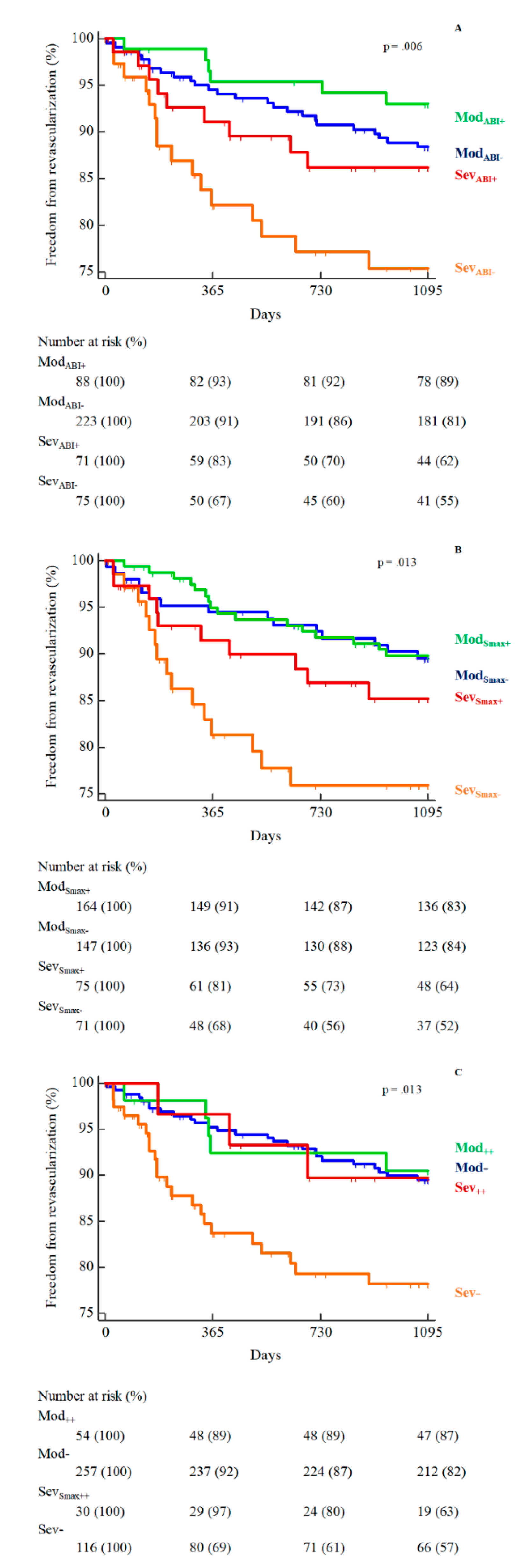
3.2. Primary Outcome: PAD-Related Revascularizations
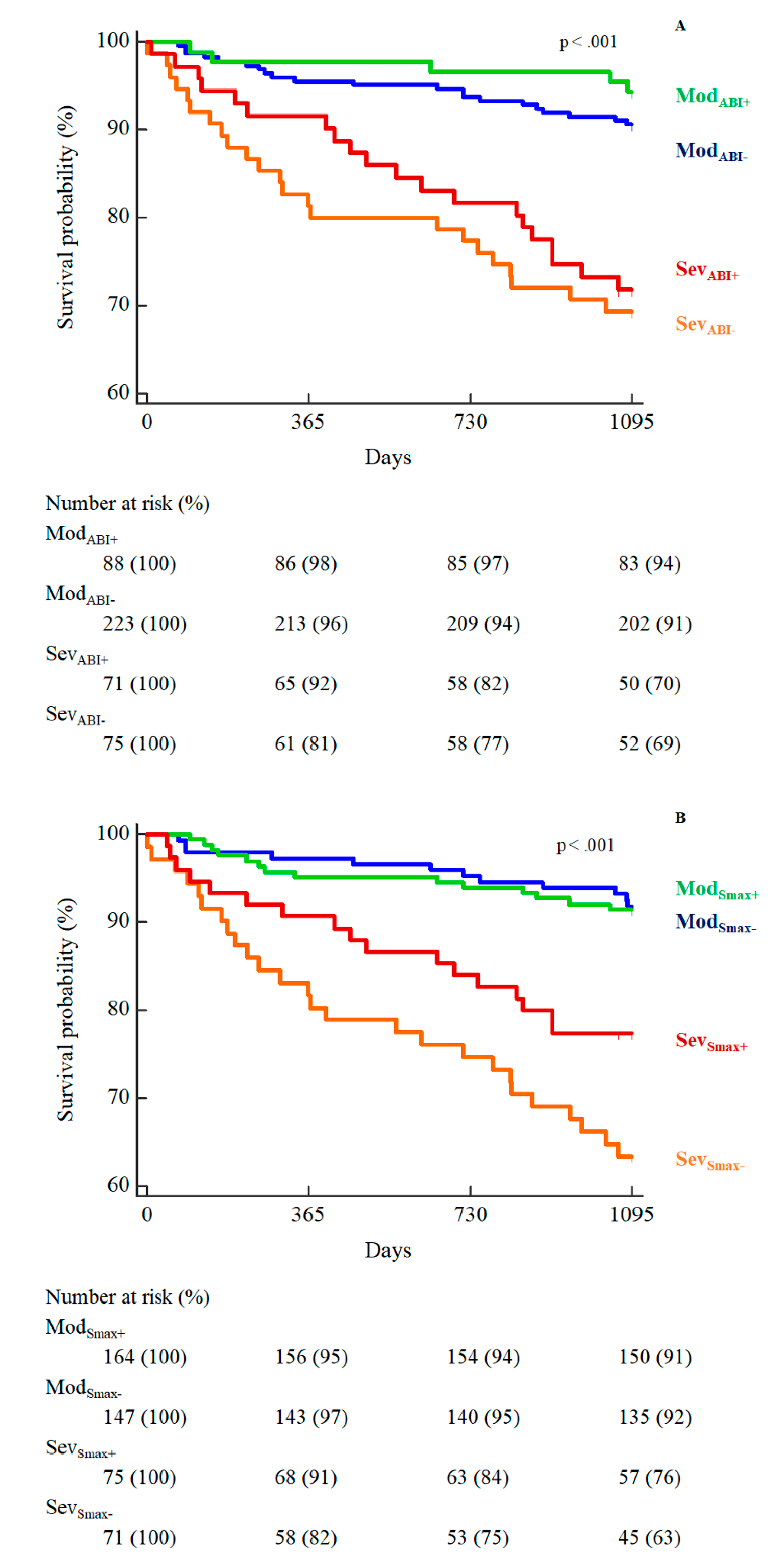
3.3. Secondary Outcome
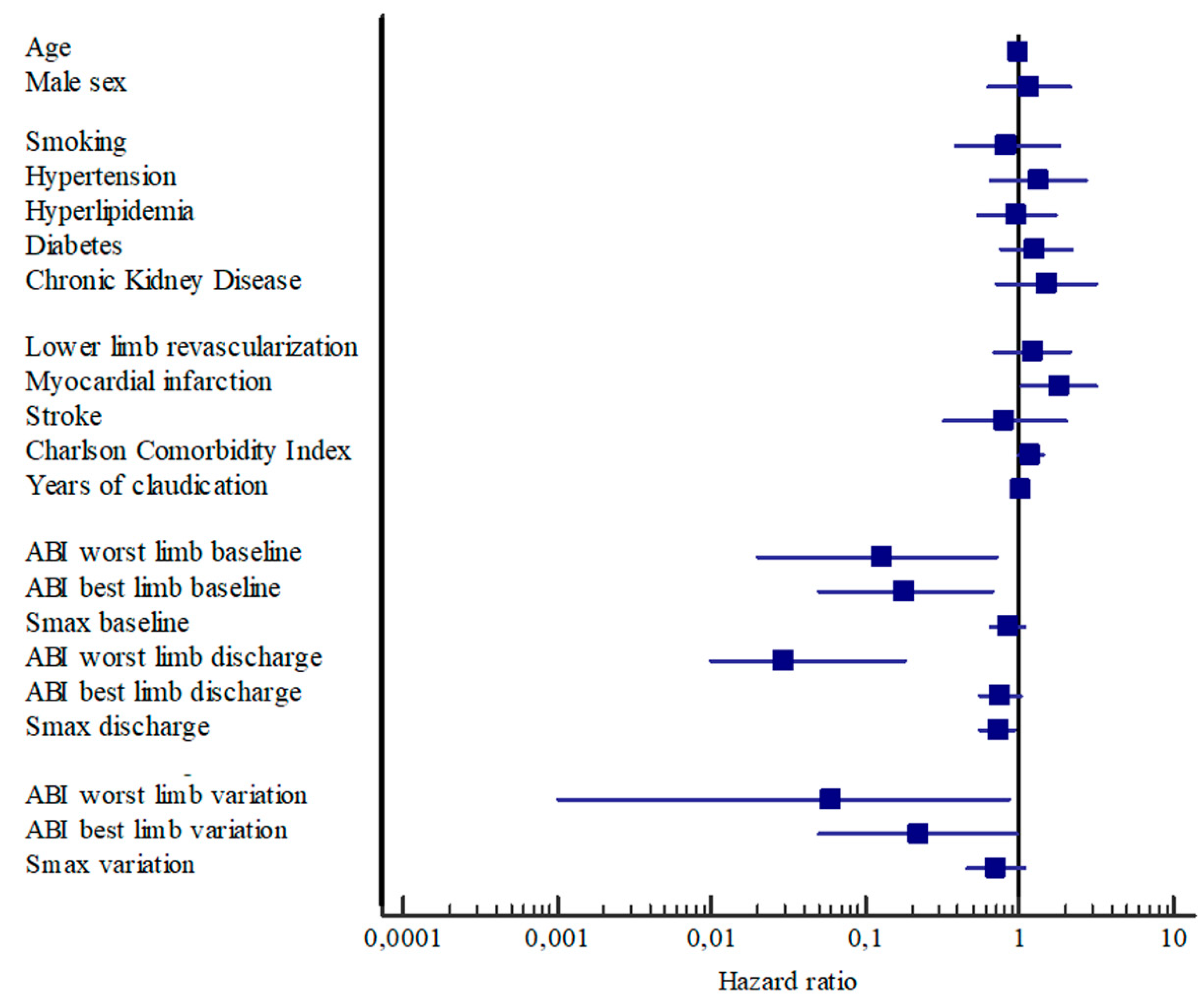
3.4. Predictors of Revascularization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Writing Committee Members; Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: Executive Summary. Vasc. Med. 2017, 22, NP1–NP43. [Google Scholar] [CrossRef] [PubMed]
- Olin, J.W.; White, C.J.; Armstrong, E.J.; Kadian-Dodov, D.; Hiatt, W.R. Peripheral Artery Disease: Evolving Role of Exercise, Medical Therapy, and Endovascular Options. J. Am. Coll. Cardiol. 2016, 67, 1338–1357. [Google Scholar] [CrossRef]
- McKenna, M.; Wolfson, S.; Kuller, L. The ratio of ankle and arm arterial pressure as an independent predictor of mortality. Atherosclerosis 1991, 87, 119–128. [Google Scholar] [CrossRef]
- Diehm, C.; Lange, S.; Darius, H.; Pittrow, D.; von Stritzky, B.; Tepohl, G.; Haberl, R.L.; Allenberg, J.R.; Dasch, B.; Trampisch, H.J. Association of low ankle brachial index with high mortality in primary care. Eur. Heart J. 2006, 27, 1743–1749. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Ninomiya, J.K.; Wingard, D.L.; Ji, M.; Fronek, A. Progression of peripheral arterial disease predicts cardiovascular disease morbidity and mortality. J. Am. Coll. Cardiol. 2008, 52, 1736–1742. [Google Scholar] [CrossRef]
- Li, X.; Luo, Y.; Xu, Y.; Li, J.; Hu, D. Relationship of ankle-brachial index with all-cause mortality and cardiovascular mortality after a 3-year follow-up: The China ankle-brachial index cohort study. J. Hum. Hypertens. 2010, 24, 111–116. [Google Scholar] [CrossRef]
- Monreal, M.; Alvarez, L.; Vilaseca, B.; Coll, R.; Suárez, C.; Toril, J.; Sanclemente, C.; FRENA Investigators. Clinical outcome in patients with peripheral artery disease. Results from a prospective registry (FRENA). Eur. J. Intern. Med. 2008, 19, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Killewich, L.A. Lack of functional benefits following infrainguinal bypass in peripheral arterial occlusive disease patients. Vasc. Med. 2001, 6, 9–14. [Google Scholar] [CrossRef]
- McDermott, M.M.; Kibbe, M.; Guralnik, J.M.; Pearce, W.H.; Tian, L.; Liao, Y.; Zhao, L.; Criqui, M.H. Comparative effectiveness study of self-directed walking exercise, lower extremity revascularization, and functional decline in peripheral artery disease. J. Vasc. Surg. 2013, 57, 990–996.e1. [Google Scholar] [CrossRef] [PubMed]
- Mazari, F.A.; Khan, J.A.; Samuel, N.; Smith, G.; Carradice, D.; McCollum, P.C.; Chetter, I.C. Long-term outcomes of a randomized clinical trial of supervised exercise, percutaneous transluminal angioplasty or combined treatment for patients with intermittent claudication due to femoropopliteal disease. Br. J. Surg. 2017, 104, 76–83. [Google Scholar] [CrossRef]
- Lamberti, N.; Malagoni, A.M.; Ficarra, V.; Basaglia, N.; Manfredini, R.; Zamboni, P.; Mascoli, F.; Manfredini, F. Structured Home-Based Exercise Versus Invasive Treatment: A Mission Impossible? A Pilot Randomized Study in Elderly Patients With Intermittent Claudication. Angiology 2016, 67, 772–780. [Google Scholar] [CrossRef]
- McDermott, M.M.; Liu, K.; Ferrucci, L.; Tian, L.; Guralnik, J.M.; Liao, Y.; Criqui, M.H. Greater sedentary hours and slower walking speed outside the home predict faster declines in functioning and adverse calf muscle changes in peripheral arterial disease. J. Am. Coll. Cardiol. 2011, 57, 2356–2364. [Google Scholar] [CrossRef]
- Gardner, A.W.; Montgomery, P.S.; Killewich, L.A. Natural history of physical function in older men with intermittent claudication. J. Vasc. Surg. 2004, 40, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Montgomery, P.S.; Parker, D.E. Physical activity is a predictor of all-cause mortality in patients with intermittent claudication. J. Vasc. Surg. 2008, 47, 117–122. [Google Scholar] [CrossRef]
- McDermott, M.M.; Liu, K.; Ferrucci, L.; Tian, L.; Guralnik, J.M.; Liao, Y.; Criqui, M.H. Decline in functional performance predicts later increased mobility loss and mortality in peripheral arterial disease. J. Am. Coll. Cardiol. 2011, 57, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.; Harwood, A.; Watson, L.; Leng, G.C. Exercise for intermittent claudication. Cochrane Database Syst. Rev. 2017, 12, CD000990. [Google Scholar] [CrossRef] [PubMed]
- Harwood, A.E.; Smith, G.E.; Cayton, T.; Broadbent, E.; Chetter, I.C. A Systematic Review of the Uptake and Adherence Rates to Supervised Exercise Programs in Patients with Intermittent Claudication. Ann. Vasc. Surg. 2016, 34, 280–289. [Google Scholar] [CrossRef]
- Katzel, L.I.; Sorkin, J.; Bradham, D.; Gardner, A.W. Comorbidities and the entry of patients with peripheral arterial disease into an exercise rehabilitation program. J. Cardiopulm. Rehabil. 2000, 20, 165–171. [Google Scholar] [CrossRef]
- Cavalcante, B.R.; Farah, B.Q.; dos A Barbosa, J.P.; Cucato, G.G.; da Rocha Chehuen, M.; da Silva Santana, F.; Wolosker, N.; de Moraes Forjaz, C.L.; Ritti-Dias, R.M. Are the barriers for physical activity practice equal for all peripheral artery disease patients? Arch. Phys. Med. Rehabil. 2015, 96, 248–252. [Google Scholar] [CrossRef]
- McDermott, M.M.; Polonsky, T.S. Home-Based Exercise: A Therapeutic Option for Peripheral Artery Disease. Circulation 2016, 134, 1127–1129. [Google Scholar] [CrossRef]
- Manfredini, F.; Malagoni, A.M.; Mascoli, F.; Mandini, S.; Taddia, M.C.; Basaglia, N.; Manfredini, R.; Conconi, F.; Zamboni, P. Training rather than walking: The test in -train out program for home-based rehabilitation in peripheral arteriopathy. Circ. J. 2008, 72, 946–952. [Google Scholar] [CrossRef]
- Malagoni, A.M.; Vagnoni, E.; Felisatti, M.; Mandini, S.; Heidari, M.; Mascoli, F.; Basaglia, N.; Manfredini, R.; Zamboni, P.; Manfredini, F. Evaluation of patient compliance, quality of life impact and cost-effectiveness of a “test in-train out” exercise-based rehabilitation program for patients with intermittent claudication. Circ. J. 2011, 75, 2128–2134. [Google Scholar] [CrossRef]
- Manfredini, F.; Malagoni, A.M.; Mandini, S.; Felisatti, M.; Mascoli, F.; Basaglia, N.; Manfredini, R.; Mikhailidis, D.P.; Zamboni, P. Near-infrared spectroscopy assessment following exercise training in patients with intermittent claudication and in untrained healthy participants. Vasc. Endovasc. Surg. 2012, 46, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Malagoni, A.M.; Cavazza, S.; Ferraresi, G.; Grassi, G.; Felisatti, M.; Lamberti, N.; Basaglia, N.; Manfredini, F. Effects of a “test in-train out” walking program versus supervised standard rehabilitation in chronic stroke patients: A feasibility and pilot randomized study. Eur. J. Phys. Rehabil. Med. 2016, 52, 279–287. [Google Scholar] [PubMed]
- Lamberti, N.; Straudi, S.; Malagoni, A.M.; Argirò, M.; Felisatti, M.; Nardini, E.; Zambon, C.; Basaglia, N.; Manfredini, F. Effects of low-intensity endurance and resistance training on mobility in chronic stroke survivors: A pilot randomized controlled study. Eur. J. Phys. Rehabil. Med. 2017, 53, 228–239. [Google Scholar] [PubMed]
- Malagoni, A.M.; Catizone, L.; Mandini, S.; Soffritti, S.; Manfredini, R.; Boari, B.; Russo, G.; Basaglia, N.; Zamboni, P.; Manfredini, F. Acute and long-term effects of an exercise program for dialysis patients prescribed in hospital and performed at home. J. Nephrol. 2008, 21, 871–878. [Google Scholar] [PubMed]
- Manfredini, F.; Rigolin, G.M.; Malagoni, A.M.; Soffritti, S.; Boari, B.; Conconi, F.; Castoldi, G.L.; Catizone, L.; Zamboni, P.; Manfredini, R. Exercise capacity and circulating endothelial progenitor cells in hemodialysis patients. Int. J. Sports Med. 2007, 28, 368–373. [Google Scholar] [CrossRef]
- Manfredini, F.; Mallamaci, F.; D’Arrigo, G.; Baggetta, R.; Bolignano, D.; Torino, C.; Lamberti, N.; Bertoli, S.; Ciurlino, D.; Rocca-Rey, L.; et al. Exercise in Patients on Dialysis: A Multicenter, Randomized Clinical Trial. J. Am. Soc. Nephrol. 2017, 28, 1259–1268. [Google Scholar] [CrossRef]
- Torino, C.; Manfredini, F.; Bolignano, D.; Aucella, F.; Baggetta, R.; Barillà, A.; Battaglia, Y.; Bertoli, S.; Bonanno, G.; Castellino, P.; et al. Physical performance and clinical outcomes in dialysis patients: A secondary analysis of the EXCITE trial. Kidney Blood Press Res. 2014, 39, 205–211. [Google Scholar] [CrossRef]
- Sakamoto, S.; Yokoyama, N.; Tamori, Y.; Akutsu, K.; Hashimoto, H.; Takeshita, S. Patients with peripheral artery disease who complete 12-week supervised exercise training program show reduced cardiovascular mortality and morbidity. Circ. J. 2009, 73, 167–173. [Google Scholar] [CrossRef]
- Manfredini, F.; Conconi, F.; Malagoni, A.M.; Manfredini, R.; Mascoli, F.; Liboni, A.; Zamboni, P. Speed rather than distance: A novel graded treadmill test to assess claudication. Eur. J. Vasc. Endovasc. Surg. 2004, 28, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Rehman, J.; Li, J.; Parvathaneni, L.; Karlsson, G.; Panchal, V.R.; Temm, C.J.; Mahenthiran, J.; March, K.L. Exercise acutely increases circulating endothelial progenitor cells and monocyte-/macrophage-derived angiogenic cells. J. Am. Coll. Cardiol. 2004, 43, 2314–2318. [Google Scholar] [CrossRef] [PubMed]
- Sandri, M.; Beck, E.B.; Adams, V.; Gielen, S.; Lenk, K.; Höllriegel, R.; Mangner, N.; Linke, A.; Erbs, S.; Möbius-Winkler, S.; et al. Maximal exercise, limb ischemia, and endothelial progenitor cells. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sigvant, B.; Hasvold, P.; Kragsterman, B.; Falkenberg, M.; Johansson, S.; Thuresson, M.; Nordanstig, J. Cardiovascular outcomes in patients with peripheral arterial disease as an initial or subsequent manifestation of atherosclerotic disease: Results from a Swedish nationwide study. J. Vasc. Surg. 2017, 66, 507–514.e1. [Google Scholar] [CrossRef] [PubMed]
- Baubeta Fridh, E.; Andersson, M.; Thuresson, M.; Sigvant, B.; Kragsterman, B.; Johansson, S.; Hasvold, P.; Falkenberg, M.; Nordanstig, J. Amputation Rates, Mortality, and Pre-operative Comorbidities in Patients Revascularised for Intermittent Claudication or Critical Limb Ischaemia: A Population Based Study. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Sigvant, B.; Lundin, F.; Wahlberg, E. The Risk of Disease Progression in Peripheral Arterial Disease is Higher than Expected: A Meta-Analysis of Mortality and Disease Progression in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Leeper, N.J.; Myers, J.; Zhou, M.; Nead, K.T.; Syed, A.; Kojima, Y.; Caceres, R.D.; Cooke, J.P. Exercise capacity is the strongest predictor of mortality in patients with peripheral arterial disease. J. Vasc. Surg. 2013, 57, 728–733. [Google Scholar] [CrossRef]
- Feringa, H.H.; Karagiannis, S.E.; Schouten, O.; Vidakovic, R.; van Waning, V.H.; Boersma, E.; Welten, G.; Bax, J.J.; Poldermans, D. Prognostic significance of declining ankle-brachial index values in patients with suspected or known peripheral arterial disease. Eur. J. Vasc. Endovasc. Surg. 2007, 34, 206–213. [Google Scholar] [CrossRef]
- Manfredini, R.; Lamberti, N.; Manfredini, F.; Straudi, S.; Fabbian, F.; Rodriguez Borrego, M.A.; Basaglia, N.; Carmona Torres, J.M.; Lopez Soto, P.J. Gender Differences in Outcomes Following a Pain-Free, Home-Based Exercise Program for Claudication. J. Womens Health (Larchmt) 2018. [Google Scholar] [CrossRef]
- Lamberti, N.; Straudi, S.; Lissia, E.; Cavazzini, L.; Buja, S.; Manfredini, R.; Basaglia, N.; Manfredini, F. Home-based exercise for elderly patients with intermittent claudication limited by osteoarticular disorders —Feasibility and effectiveness of a low-intensity program. Vasa 2018, 47, 227–234. [Google Scholar] [CrossRef]
- Höbaus, C.; Herz, C.T.; Obendorf, F.; Howanietz, M.T.; Wrba, T.; Koppensteiner, R.; Schernthaner, G.H. Center-based patient care enhances survival of elderly patients suffering from peripheral arterial disease. Ann. Med. 2017, 49, 291–298. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Moderate (n = 311) | Severe (n = 146) | p | |
|---|---|---|---|
| Male sex | 223 (72) | 110 (75) | 0.41 |
| Age, years | 71 ± 6 | 72 ± 5 | 0.07 |
| Sedentary occupation | 209 (67) | 89 (61) | 0.19 |
| Risk factors; n (%) | |||
| Smoking | 277 (89) | 134 (92) | 0.37 |
| Hypertension | 247 (79) | 121 (83) | 0.38 |
| Hyperlipidemia | 218 (70) | 103 (71) | 0.92 |
| Diabetes mellitus | 119 (38) | 54 (37) | 0.79 |
| Chronic Kidney Disease | 30 (10) | 20 (14) | 0.20 |
| Familiarity for CVD | 72 (23) | 35 (24) | 0.85 |
| Comorbidities; n (%) | |||
| Chronic Heart Disease | 123 (40) | 63 (43) | 0.47 |
| Stroke | 35 (11) | 16 (11) | 0.93 |
| Osteoarticular disease | 78 (25) | 35 (24) | 0.80 |
| Pulmonary disease | 18 (6) | 15 (10) | 0.08 |
| Neoplastic disease | 25 (8) | 14 (10) | 0.58 |
| Charlson Comorbidity Index | 2.6 ± 1.4 | 2.7 ± 1.5 | 0.51 |
| Age-adjusted Charlson Index | 6.2 ± 1.5 | 6.4 ± 1.6 | 0.27 |
| Peripheral artery disease | |||
| Grade I—Category 1 | 168 (54) | 31 (21) | <0.001 |
| Grade I—Category 2 | 118 (38) | 55 (38) | <0.001 |
| Grade I—Category 3 | 25 (8) | 60 (41) | <0.001 |
| Self-reported claudication distance (m) | 209 ± 187 | 114 ± 121 | <0.001 |
| Lower limbs revascularization | 85 (27) | 49 (34) | 0.17 |
| Disease duration, years | 6 ± 6 | 7 ± 6 | 0.09 |
| Bilateral disease | 206 (66) | 119 (82) | <0.001 |
| ABI more impaired limb | 0.64 ± 0.08 | 0.39 ± 0.10 | <0.001 |
| ABI less impaired limb | 0.86 ± 0.16 | 0.66 ± 0.22 | <0.001 |
| PTS (km/h) | 2.9 ± 1.1 | 2.5 ± 0.9 | <0.001 |
| Smax (km/h) | 3.4 ± 1.1 | 3.0 ± 1.0 | <0.001 |
| Moderate (n = 311) | Severe (n = 146) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | End | ∆ | p Within-Group | Baseline | End | ∆ | p Within-Group | Between-Group ∆ in Changes | p Between-Group | |
| ABI worst leg | 0.64 (0.63–0.65) | 0.69 (0.67–0.70) | 0.04 (0.03–0.05) | <0.001 | 0.39 (0.38–0.41) | 0.50 (0.48–0.52) | 0.11 (0.09–0.12) | <0.001 | 0.06 (0.04–0.08) | <0.001 |
| ABI best leg | 0.86 (0.84–0.88) | 0.89 (0.88–0.90) | 0.03 (0.02–0.04) | <0.001 | 0.66 (0.63–0.70) | 0.72 (0.68–0.76) | 0.06 (0.03–0.09) | <0.001 | 0.03 (0.01–0.05) | <0.001 |
| PTS (km/h) | 2.9 (2.8–3.0) | 3.7 (3.5–3.8) | 0.8 (0.7–0.9) | <0.001 | 2.4 (2.3–2.6) | 3.1 (3.0–3.3) | 0.7 (0.6–0.8) | <0.001 | 0.1 (−0.1–0.2) | 0.23 |
| Smax(km/h) | 3.4 (3.3–3.6) | 4.0 (3.8–4.1) | 0.5 (0.4–0.6) | <0.001 | 3.0 (2.9–3.2) | 3.4 (3.3–3.6) | 0.4 (0.3–0.5) | <0.001 | 0.1 (−0.2–0.2) | 0.10 |
| Whole Population (n = 457) | Moderate (n = 311) | Severe (n = 146) | ||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | Univariate | Multivariate | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Age | 0.99 (0.94–1.04) | 0.97 (0.91–1.03) | 1.01 (0.93–1.08) | |||
| Male sex | 1.15 (0.63–2.12) | 1.76 (0.72–4.30) | 0.64 (0.28–1.50) | |||
| Smoking | 0.83 (0.38–1.83) | 0.86 (0.30–2.46) | 0.72 (0.21–2.39) | |||
| Hypertension | 1.31 (0.64–2.69) | 1.36 (0.52–3.56) | 1.16 (0.40–3.39) | |||
| Hyperlipidemia | 0.96 (0.54–1.69) | 1.75 (0.71–4.26) | 0.52 (0.24–1.15) | 0.24 (0.10–0.60) | ||
| Diabetes mellitus | 1.27 (0.74–2.15) | 1.57 (0.78–3.19) | 0.95 (0.42–2.14) | |||
| Chronic Kidney Disease | 1.50 (0.71–3.18) | 2.50 (1.03–6.12) | 2.99 (1.20–7.45) | 0.60 (0.14–2.54) | ||
| Lower limbs revascularization | 1.21 (0.69–2.12) | 1.81 (0.88–3.72) | 0.62 (0.25–1.57) | |||
| Myocardial infarction | 1.80 (1.02–3.19) | 1.90 (1.07–3.36) | 1.75 (0.82–3.73) | 2.20 (0.92–5.27) | 3.63 (1.44–9.14) | |
| Stroke | 0.79 (0.31–1.99) | 0.89 (0.27–2.93) | 0.66 (0.16–2.79) | |||
| Charlson Comorbidity Index | 1.19 (1.00–1.42) | 1.22 (0.97–1.54) | 1.12 (0.88–1.45) | |||
| Disease duration | 1.02 (0.98–1.06) | 0.99 (0.93–1.06) | 1.04 (0.99–1.10) | |||
| ABI worst limb baseline | 0.13 (0.02–0.70) | 0.21 (0.002–20.62) | 1.52 (0.02–82.29) | |||
| ABI best limb baseline | 0.18 (0.05–0.66) | 3.46 (0.42–28.60) | 0.06 (0.01–0.44) | 0.02 (0.001–0.22) | ||
| Smax baseline | 0.84 (0.65–1.07) | 0.92 (0.67–1.27) | 0.81 (0.54–1.21) | |||
| ABI worst limb discharge | 0.03 (0.006–0.18) | 0.03 (0.004–0.16) | 0.05 (0.002–0.98) | 0.02 (0.001–0.42) | 0.04 (0.002–0.93) | |
| ABI best limb discharge | 0.76 (0.55–1.02) | 0.64 (0.33–1.16) | 0.82 (0.24–2.92) | |||
| Smax discharge | 0.72 (0.56–0.93) | 0.85 (0.59–1.21) | 0.69 (0.47–1.01) | 0.57 (0.37–0.89) | ||
| Δ ABI worst limb | 0.06 (0.004–0.84) | 0.03 (0.001–1.29) | 0.01 (0.0002–0.45) | 0.003 (0.0001–0.09) | ||
| Δ ABI best limb | 0.22 (0.05–0.97) | 0.20 (0.04–1.47) | 0.23 (0.03–1.66) | |||
| Δ Smax | 0.70 (0.45–1.08) | 0.85 (0.49–1.49) | 0.57 (0.29–1.14) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredini, F.; Lamberti, N.; Guerzoni, F.; Napoli, N.; Gasbarro, V.; Zamboni, P.; Mascoli, F.; Manfredini, R.; Basaglia, N.; Rodríguez-Borrego, M.A.; et al. Rehabilitative Exercise Reduced the Impact of Peripheral Artery Disease on Vascular Outcomes in Elderly Patients with Claudication: A Three-Year Single Center Retrospective Study. J. Clin. Med. 2019, 8, 210. https://doi.org/10.3390/jcm8020210
Manfredini F, Lamberti N, Guerzoni F, Napoli N, Gasbarro V, Zamboni P, Mascoli F, Manfredini R, Basaglia N, Rodríguez-Borrego MA, et al. Rehabilitative Exercise Reduced the Impact of Peripheral Artery Disease on Vascular Outcomes in Elderly Patients with Claudication: A Three-Year Single Center Retrospective Study. Journal of Clinical Medicine. 2019; 8(2):210. https://doi.org/10.3390/jcm8020210
Chicago/Turabian StyleManfredini, Fabio, Nicola Lamberti, Franco Guerzoni, Nicola Napoli, Vincenzo Gasbarro, Paolo Zamboni, Francesco Mascoli, Roberto Manfredini, Nino Basaglia, María Aurora Rodríguez-Borrego, and et al. 2019. "Rehabilitative Exercise Reduced the Impact of Peripheral Artery Disease on Vascular Outcomes in Elderly Patients with Claudication: A Three-Year Single Center Retrospective Study" Journal of Clinical Medicine 8, no. 2: 210. https://doi.org/10.3390/jcm8020210