Orbital and Eyelid B-Cell Lymphoma: A Multicenter Retrospective Study

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Collected Data
2.3. Statistical Analysis
3. Results
3.1. Clinical Features
3.2. Treatment
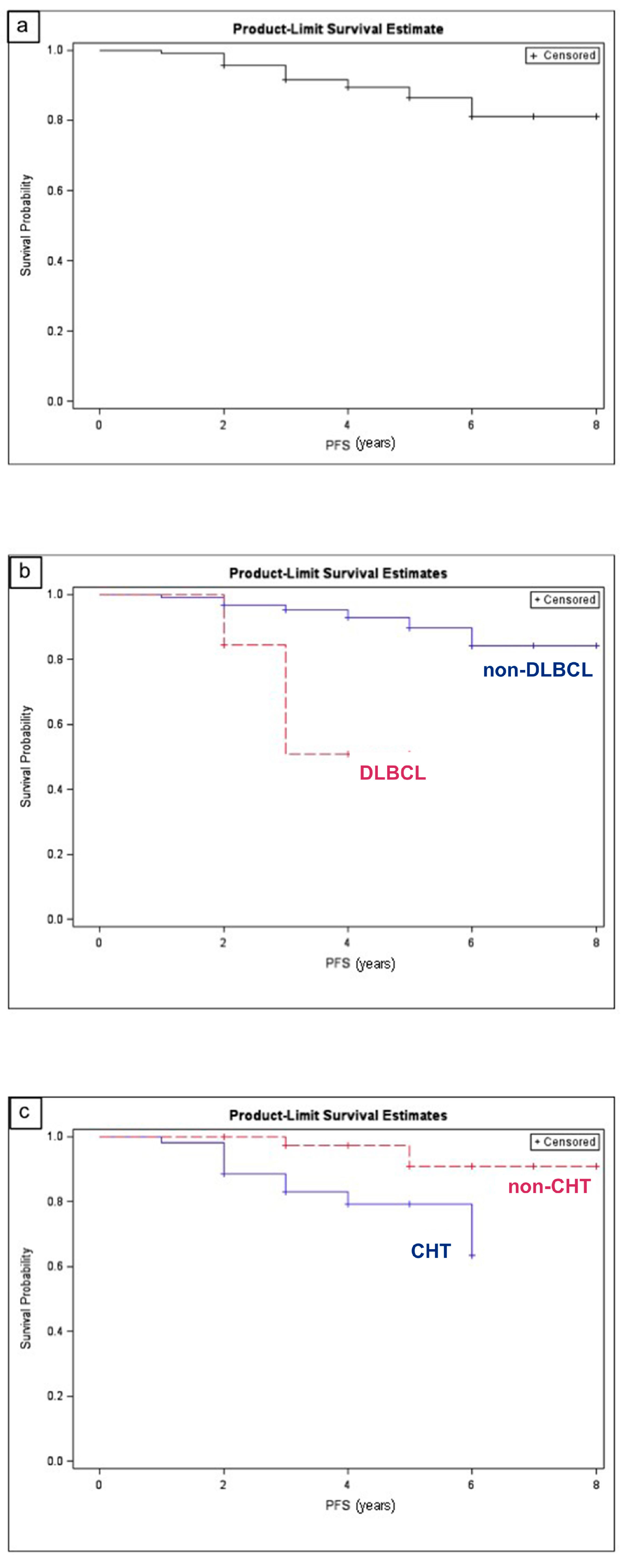
3.3. Treatment Outcome and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferry, J.A.; Fung, C.Y.; Zukerberg, L.; Lucarelli, M.J.; Hasserjian, R.P.; Preffer, F.I.; Harris, N.L. Lymphoma of the ocular adnexa: A study of 353 cases. Am. J. Surg. Pathol. 2007, 31, 170–184. [Google Scholar] [CrossRef]
- Sjo, L.D. Ophthalmic lymphoma: Epidemiology and pathogenesis. Acta Ophthalmol. 2009, 87, 1–20. [Google Scholar]
- Svendsen, F.H.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; Khong, J.J.; McKelvie, P.A.; et al. Lymphoma of the Eyelid—An International Multicenter Retrospective Study. Am. J. Ophthalmol. 2017, 77, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.G.; Holm, F.; Mikkelsen, L.H.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; et al. Orbital Lymphoma—An International Multicenter Retrospective Study. Am. J. Ophthalmol. 2019, 199, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Tanenbaum, R.E.; Galor, A.; Dubovy, S.R.; Karp, C.L. Classification, diagnosis, and management of conjunctival lymphoma. Eye Vis. 2019, 6, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrella, T.; Bron, A.; Foulet, A.; Arnould, L.; Chirpaz, L.; Michiels, R. Report of a Primary Lymphoma of the Conjunctiva: A Lymphoma of MALT Origin? Pathol. Res. Pract. 1991, 187, 78–84. [Google Scholar] [CrossRef]
- Cho, E.Y.; Han, J.J.; Ree, H.J.; Ko, Y.H.; Kang, Y.K.; Ahn, H.S.; Ahn, S.D.; Park, C.J.; Huh, J. Clinicopathologic analysis of ocular adnexal lymphomas: Extranodal marginal zone b-cell lymphoma constitutes the vast majority of ocular lymphomas among Koreans and affects younger patients. Am. J. Hematol. 2003, 73, 87–96. [Google Scholar] [CrossRef]
- Bardenstein, D.S. Ocular adnexal lymphoma: Classification, clinical disease, and molecular biology. Ophthalmol. Clin. N. Am. 2005, 18, 187–197. [Google Scholar] [CrossRef]
- Rubinstein, T.J.; Aziz, H.A.; Bellerive, C.; Sires, B.S.; Hing, A.W.; Habermehl, G.; Hsi, E.; Singh, A.D. Ocular/adnexal lymphoma: Dissimilar to systemic lymphoma. Surv. Ophthalmol. 2017, 63, 381–388. [Google Scholar] [CrossRef]
- Harris, N.L.; Stein, H.; Coupland, S.E.; Hummel, M.; Favera, R.D.; Pasqualucci, L.; Chan, W.C. New approaches to lymphoma diagnosis. Hematology 2001, 194–220. [Google Scholar] [CrossRef] [Green Version]
- Vega, F.; Medeiros, L.J. Chromosomal translocations involved in non-Hodgkin lymphomas. Arch. Pathol. Lab. Med. 2003, 127, 1148–1160. [Google Scholar]
- Coupland, S.E. Molecular pathology of lymphoma. Eye 2003, 27, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decaudin, D.; de Cremoux, P.; Vincent-Salomon, A.; Dendale, R.; Rouic, L.L. Ocular adnexal lymphoma: Clinicopathologic features and treatment options. Blood 2006, 108, 1451–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharara, N.; Holden, J.T.; Wojno, T.H.; Feinberg, A.S.; Grossniklaus, H.E. Ocular adnexa lymphoid proliferations: Clinical, histologic, flow cytometric, and molecular analysis of forty-three cases. Ophthalmology 2003, 110, 1245–1254. [Google Scholar] [CrossRef]
- Streubel, B.; Simonitsch-Klupp, I.; Mullauer, L.; Lamprecht, A.; Huber, D.; Siebert, R.; Stolte, M.; Trautinger, F.; Lukas, J.; Püspök, A.; et al. Variable frequencies of MALT lymphoma-associated genetic aberrations in MALT lymphomas of different sites. Leukemia 2004, 18, 1722–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Streubel, B.; Vinatzer, U.; Lamprecht, A.; Raderer, M.; Chott, A. t(3;14)(p14.1;q32) involving IGH and FOXP1 is a novel recurrent chromosomal aberration in MALT lymphoma. Leukemia 2005, 19, 652–658. [Google Scholar] [CrossRef]
- Ye, H.; Liu, H.; Attygale, A.; Wotherspoon, A.C.; Nicholson, A.G.; Charlotte, F.; Leblond, V.; Speight, P.; Goodlad, J.; Lavergne-Slove, A.; et al. Variable frequencies of t(11;18)(q21:q21) in MALT lymphomas of different sites: Significant association with CagA strains of H pylori in gastric MALT lymphoma. Blood 2003, 102, 1012–1018. [Google Scholar] [CrossRef]
- Chen, P.M.; Chiou, T.J.; Yu, I.T.; Fan, F.S.; Chu, C.J.; Kao, S.C.; Wang, W.S.; Liu, J.H.; Hsu, W.M.; Yang, M.H.; et al. Molecular analysis of mucosa-associated lymphoid tissue (MALT) lymphoma of ocular adnexa. Leuk. Lymphoma 2001, 42, 207–214. [Google Scholar] [CrossRef]
- Biagi, J.J.; Seymour, J.F. Insights into the molecular pathogenesis of follicular lymphoma arising from analysis of geographic variation. Blood 2002, 99, 4265–4275. [Google Scholar] [CrossRef]
- Rasmussen, P.K.; Coupland, S.E.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; McKelvie, P.; Mulay, K.; Prause, J.U.; Ralfkiaer, E.; et al. Ocular adnexal follicular lymphoma: A multicenter international study. JAMA Ophthalmol. 2014, 132, 851–858. [Google Scholar] [CrossRef]
- Rasmussen, P.; Ralfkiaer, E.; Prause, J.U.; Sjö, L.D.; Specht, L.; Rossing, H.H.; Siersma, V.D.; Heegaard, S. Follicular lymphoma of the ocular adnexal region: A nation-based study. Acta Ophthalmol. 2015, 93, 184–191. [Google Scholar] [CrossRef]
- Raffeld, M.; Jaffe, E.S. Bcl-1, t(11;14), and mantle cell-derived lymphomas. Blood 1991, 78, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Looi, A.; Gascoyne, R.D.; Chhanabhai, M.; Connors, J.M.; Rootman, J.; White, V.A. Mantle cell lymphoma in the ocular adnexal region. Ophthalmology 2005, 112, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, M.K.H.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Khong, J.J.; McKelvie, P.A.; Mulay, K.; et al. Clinicopathological features of ocular adnexal mantle-cell lymphoma in an international multicenter cohort. JAMA Ophthalmol. 2017, 135, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Coupland, S.E.; Krause, L.; Delecluse, H.J.; Anagnostopoulos, I.; Foss, H.D.; Hummel, M.; Bornfeld, N.; Lee, W.R.; Stein, H. Lymphoproliferative lesions of the ocular adnexa. Analysis of 112 cases. Ophthalmology 1998, 105, 1430–1441. [Google Scholar] [CrossRef]
- Offit, K.; Lo Coco, F.; Louie, D.C.; Parsa, N.Z.; Leung, D.; Portlock, C.; Ye, B.H.; Lista, F.; Filippa, D.A.; Rosenbaum, A. Rearrangement of the bcl-6 gene as a prognostic marker in diffuse large-cell lymphoma. N. Engl. J. Med. 1994, 331, 74–80. [Google Scholar] [CrossRef]
- Kramer, M.H.; Hermans, J.; Wijburg, E.; Philippo, K.; Geelen, E.; van Krieken, J.H.; de Jong, D.; Maartense, E.; Schuuring, E.; Kluin, P.M. Clinical relevance of BCL2, BCL6, and MYC rearrangements in diffuse large B-cell lymphoma. Blood 1998, 92, 3152–3162. [Google Scholar] [CrossRef]
- Wierda, W.G.; Byrd, J.C.; Abramson, J.S.; Bilgrami, S.F.; Bociek, G.; Brander, D.; Brown, J.; Chanan-Khan, A.A.; Chavez, J.C.; Coutre, S.E.; et al. NCCN Guidelines Insights: Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma, Version 2.2019. J. Natl. Compr. Canc. Netw. 2019, 17, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Kastenbaum, H.A.; Khalbuss, W.E.; Felgar, R.E.; Stoller, R.; Monaco, S.E. The spectrum of coincident entities with small lymphocytic lymphoma/chronic lymphocytic leukemia (SLL/CLL) diagnosed by cytology. Cytojournal 2010, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, M.M.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; Khong, J.J.; McKelvie, P.A.; et al. Conjunctival Lymphoma—An International Multicenter Retrospective Study. JAMA Ophthalmol. 2016, 134, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Esmaeli, B.; Sniegowski, M. Orbital and ocular adnexal lymphoma. In Orbital Tumors: Diagnosis and Treatment; Karcioglu, Z.A., Ed.; Springer: New York, NY, USA, 2015. [Google Scholar]
- Collina, F.; De Chiara, A.; De Renzo, A.; De Rosa, G.; Botti, G.; Franco, R. Chlamydia psittaci in ocular adnexa MALT lymphoma: A possible role in lymphomagenesis and a different geographical distribution. Infect. Agent. Cancer 2012, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Chanudet, E.; Zhou, Y.; Bacon, C.M.; Wotherspoon, A.C.; Müller-Hermelink, H.K.; Adam, P.; Dong, H.Y.; de Jong, D.; Li, Y.; Wei, R.; et al. Chlamydia psittaci is variably associated with ocular adnexal MALT lymphoma in different geographical regions. J. Pathol. 2006, 209, 344–351. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New, York, NY, USA; American Joint Commission on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Mancuso, S.; Carlisi, M.; Santoro, M.; Napolitano, M.; Raso, S.; Siragusa, S. Immunosenescence and lymphomagenesis. Immun. Ageing 2018, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Cohen, V.M.L.; Sweetenham, J.; Singh, A.D. Ocular adnexal lymphoma. What is the evidence for an infectious aetiology? Br. J. Ophthalmol. 2008, 92, 446–448. [Google Scholar] [CrossRef] [PubMed]
- Strianese, D.; Tranfa, F.; Finelli, M.; De Renzo, A.; Staibano, S.; Schiemer, R.; Cardone, D.; Pacelli, R.; Perna, F.; Mascolo, M.; et al. Hepatitis C virus infection in ocular adnexal lymphomas. Arch. Ophthalmol. 2010, 128, 1295–1299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkelsen, L.H.; Würtz, N.S.; Heegaard, S. Recent advances in treating extraocular lymphomas. Expert Rev. Ophthalmol. 2018, 13, 205–217. [Google Scholar] [CrossRef]
- Sassone, M.; Ponzoni, M.; Ferreri, A.J. Ocular adnexal marginal zone lymphoma: Clinical presentation, pathogenesis, diagnosis, prognosis, and treatment. Best Pr. Res. Clin. Haematol. 2017, 30, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Platt, S.; Zahrani, Y.A.; Singh, N.; Hill, B.; Cherian, S.; Singh, A.D. Extranodal marginal zone lymphoma of ocular adnexa: Outcomes following radiation therapy. Ocul. Oncol. Pathol. 2017, 3, 181–187. [Google Scholar] [CrossRef]
- Tsang, R.W.; Gospodarowicz, M.K.; Pintilie, M.; Wells, W.; Hodgson, D.C.; Sun, A.; Crump, M.; Patterson, B.J. Localized mucosa-associated lymphoid tissue lymphoma treated with radiation therapy has excellent clinical outcome. J. Clin. Oncol. 2003, 21, 4157–4164. [Google Scholar] [CrossRef]
- Hindsø, T.G.; Esmaeli, B.; Holm, F.; Mikkelsen, L.H.; Rasmussen, P.K.; Coupland, S.E.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; et al. International multicentre retrospective cohort study of ocular adnexal marginal zone B-cell lymphoma. Br. J. Ophthalmol. 2020, 104, 357–362. [Google Scholar] [CrossRef]
- Yen, M.T.; Bilyk, J.R.; Wladis, E.J.; Bradley, E.A.; Mawn, L.A. Treatments for ocular adnexal lymphoma: A report by the american academy of ophthalmology. Ophthalmology 2018, 125, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Dreyling, M.; Thieblemont, C.; Gallamini, A.; Arcaini, L.; Campo, E.; Hermine, O.; Kluin-Nelemans, J.C.; Ladetto, M.; Le Gouill, S.; Iannitto, E.; et al. ESMO Consensus conferences: Guidelines on malignant lymphoma. part 2: Marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann. Oncol. 2013, 24, 857–877. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, P.; Sjo, L.D.; Prause, J.U.; Ralfkiaer, E.; Heegaard, S. Mantle cell lymphoma in the orbital and adnexal region. Br. J. Ophthalmol. 2009, 93, 1047–1051. [Google Scholar] [CrossRef] [PubMed]
- Dreyling, M.; Ghielmini, M.; Rule, S.; Salles, G.; Vitolo, U.; Ladetto, M. ESMO Guidelines Committee. Newly diagnosed and relapsed follicular lymphoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, 3109. [Google Scholar] [CrossRef] [PubMed]
- Munch-Petersen, H.D.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G.; Khong, J.J.; McKelvie, P.A.; et al. Ocular adnexal diffuse large B-cell lymphoma a multicenter international study. JAMA Ophthalmol. 2015, 133, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; International Agency for Research in Cancer (IARC): Lyon, France, 2008; pp. 1–439. [Google Scholar]
- Rasmussen, P.; Ralfkiaer, E.; Prause, J.U.; Sjö, L.D.; Toft, P.B.; Siersma, V.D.; Heegaard, S. Diffuse large B-cell lymphoma of the ocular adnexal region: A nation-based study. Acta Ophthalmol. 2013, 91, 163–169. [Google Scholar] [CrossRef]
- Stacy, R.C.; Jakobiec, F.A.; Herwig, M.C.; Schoenfield, L.; Singh, A.; Grossniklaus, H.E. Diffuse large B-cell lymphoma of the orbit: Clinicopathologic, immunohistochemical, and prognostic features of 20 cases. Am. J. Ophthalmol. 2012, 154, 87–98. [Google Scholar] [CrossRef]
- Esmaeli, B.; Murray, J.L.; Ahmadi, M.A.; Naderi, A.; Singh, S.; Romaguera, J.; White, C.A.; McLaughlin, P. Immunotherapy for low-grade non-hodgkin secondary lymphoma of the orbit. Arch. Ophthalmol. 2002, 120, 1225–1227. [Google Scholar]
- Aronow, M.D.; Portell, C.A.; Rybicki, L.A.; Macklis, R.; Singh, A.D.; Sweetenham, J.W. Ocular Adnexal Lymphoma: Assessment of a Tumor-Node-Metastasis Staging System. Ophthalmology 2013, 120, 1915–1919. [Google Scholar] [CrossRef]
- Graue, G.F.; Finger, P.T.; Maher, E.; Della Rocca, D.; Della Rocca, R.; Lelli, G.J., Jr.; Milman, T. Ocular adnexal lymphoma staging and treatment: American Joint Committee on Cancer versus Ann Arbor. Eur. J. Ophthalmol. 2013, 23, 344–355. [Google Scholar] [CrossRef]
- Kattan, M.W.; Hess, K.R.; Amin, M.B.; Lu, Y.; Moons, K.G.; Gershenwald, J.E.; Gimotty, P.A.; Guinney, J.H.; Halabi, S.; Lazar, A.J.; et al. American joint committee on cancer acceptance criteria for inclusion of risk models for individualized prognosis in the practice of precision medicine. CA Cancer J. Clin. 2016, 66, 370–374. [Google Scholar] [CrossRef] [Green Version]
- Kwon, M.; Lee, J.S.; Lee, C.; Yoon, D.H.; Sa, H.S. Prognostic factors for relapse and survival among patients with ocular adnexal lymphoma: Validation of the eighth edition of the American Joint Committee on Cancer (AJCC) TNM classification. Br. J. Ophthalmol. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Lymphoma Subtypes | Genetic Alterations |
|---|---|
| EMZL | - t(11;18)(q21;q21)in 15–40% [15] - t(14;18)(q32;q21) in 24% [15] - t(3;14)(p14.1;q32) in 20% [16,17,18] - Trisomy 3, 18 [16,17,18] |
| FL | - t(14;18)(q32;q21) in 76%, resulting in the expression of BCL-2 [19,20] - p53 gene mutations and c-myc rearrangement in high-grade cases [20,21] |
| MCL | - t(11;14)(q13;q32) in almost all cases, resulting in cyclin D1 overexpression [22,23,24] - p53 gene mutations and c-myc rearrangement in high-grade cases [22,23,24] |
| DLBCL | - Bcl-6 gene rearrangements in 40% [24] - Bcl-2 gene rearrangements in 25% [24] - C-myc gene rearrangements extremely rare [25,26] |
| SLL | - del(13q) in 55% [28,29] - Trisomy 12 [28,29] |
| Clinical Features and Histopathologic Subtypes | EMZL | SLL | DLBCL | FL | MCL | BL |
|---|---|---|---|---|---|---|
| No. of patients | 93 | 18 | 13 | 9 | 6 | 2 |
| Gender (Male:Female) | 47:46 | 10:8 | 8:5 | 4:5 | 5:1 | 1:1 |
| Median age at presentation (SD) | 65 (8.3) | 66 (9.2) | 68 (5.6) | 66 (9.1) | 71 (3.1) | 40 (0.5) |
| Laterality (Unilateral:Bilateral) | 87:6 | 13:5 | 13:0 | 18:0 | 4:2 | 2:0 |
| Location: | ||||||
| - Orbital tissue | 76 | 18 | 11 | 9 | 4 | 2 |
| - Lacrimal gland | 14 | - | 2 | - | 2 | - |
| - Eyelid | 3 | - | - | - | - | - |
| Disease presentation: | ||||||
| - Primary OEL | 86 | 16 | 8 | 9 | 5 | - |
| - Secondary OEL | 7 | 2 | 5 | - | - | 2 |
| No. of patients with risk factors: | 17 | 4 | 7 | 5 | - | - |
| Symptoms: | ||||||
| - Mass | 80 | 7 | 11 | 6 | 6 | 2 |
| - Swelling | 72 | 13 | 13 | 7 | 4 | 2 |
| - Proptosis | 31 | 2 | 11 | 2 | 1 | - |
| - Diplopia | 10 | 1 | 9 | 1 | - | 2 |
| - Ptosis | 14 | - | 1 | - | - | - |
| Signs: | ||||||
| - Proptosis | 47 | 9 | 11 | 3 | 4 | 2 |
| - Globe displacement | 63 | 11 | 10 | 1 | 1 | 2 |
| - Limited motility | 27 | 5 | 9 | 5 | 2 | 2 |
| - Ptosis | 34 | - | - | - | - | - |
| - Epiphora | 20 | 2 | 2 | 1 | 1 | - |
| Category | Variable | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| Median Survival Time (SD) | p-Value | HR (95%) | p-Value | ||
| Histopathology | EMZL | 60 (2) | 0.1973 | 2.853 | 0.2014 |
| SLL | 66 (3) | 0.5244 | - | - | |
| DLBCL | 36 (0.5) | 0.0004 | 8.581 | 0.0112 | |
| FL | 51 (2.5) | 0.2601 | - | - | |
| MCL | 46 (2.6) | 0.4530 | - | - | |
| BL | 36 (0.7) | 0.6703 | - | - | |
| Risk factors | HCV | 36 (1.1) | 0.3231 | - | - |
| HBV | 43 (2.1) | 0.5720 | - | - | |
| Others | 43 (3.1) | 0.3435 | - | - | |
| Treatment | EBRT | 68 (3.3) | 0.3531 | - | - |
| CHT | 63 (3.2) | 0.0025 | 9.239 | 0.0094 | |
| Immunotherapy | 60 (2.2) | 0.8556 | - | - | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savino, G.; Midena, G.; Blasi, M.A.; Battendieri, R.; Grimaldi, G.; Maceroni, M.; Tranfa, F.; Napolitano, P.; Lanni, V.; Iuliano, A. Orbital and Eyelid B-Cell Lymphoma: A Multicenter Retrospective Study. Cancers 2020, 12, 2538. https://doi.org/10.3390/cancers12092538
Savino G, Midena G, Blasi MA, Battendieri R, Grimaldi G, Maceroni M, Tranfa F, Napolitano P, Lanni V, Iuliano A. Orbital and Eyelid B-Cell Lymphoma: A Multicenter Retrospective Study. Cancers. 2020; 12(9):2538. https://doi.org/10.3390/cancers12092538
Chicago/Turabian StyleSavino, Gustavo, Giulia Midena, Maria Antonietta Blasi, Remo Battendieri, Gabriela Grimaldi, Martina Maceroni, Fausto Tranfa, Pasquale Napolitano, Vittoria Lanni, and Adriana Iuliano. 2020. "Orbital and Eyelid B-Cell Lymphoma: A Multicenter Retrospective Study" Cancers 12, no. 9: 2538. https://doi.org/10.3390/cancers12092538