Epidemiology of Hypoalbuminemia in Hospitalized Patients: A Clinical Matter or an Emerging Public Health Problem?

 ,
,  , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Limaye, K.; Yang, J.D.; Hinduja, A. Role of admission serum albumin levels in patients with intracerebral hemorrhage. Acta Neurol. Belg. 2016, 116, 27–30. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talwalkar, S.S.; Bon Homme, M.; Miller, J.J.; Elin, R.J. Ischemia modified albumin. a marker of acute ischemic events: A pilot study. Ann. Clin. Lab. Sci. 2008, 38, 132–137. [Google Scholar] [PubMed]
- Mosli, R.H.; Mosli, H.H. Obesity and morbid obesity associated with higher odds of hypoalbuminemia in adults without liver disease or renal failure. Diabetes Metab. Syndr. Obes. 2017, 10, 467–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.M.; Zhang, W.H.; Ying, H.Q.; Xu, Y.M.; Zhang, J.; Min, Q.H.; Huang, B.; Lin, J.; Chen, J.J.; Wang, X.Z. Two new inflammatory markers associated with disease activity score-28 in patients with rheumatoid arthritis: Albumin to fibrinogen ratio and C-reactive protein to albumin ratio. Int. Immunopharmacol. 2018, 62, 293–298. [Google Scholar] [CrossRef]
- Vaglio, S.; Calizzani, G.; Grazzini, G.; Lanzoni, M.; Liumbruno, G.M. Italian albumin usage (or misusage?). Eur. J. Intern. Med. 2014, 25, e31–e32. [Google Scholar] [CrossRef]
- Chang, D.C.; Xu, X.; Ferrante, A.W., Jr.; Krakoff, J. Reduced plasma albumin predicts type 2 diabetes and is associated with greater adipose tissue macrophage content and activation. Diabetol. Metab. Syndr. 2019, 11, 14. [Google Scholar] [CrossRef]
- Koga, M.; Kasayama, S. Clinical impact of glycated albumin as another glycemic control marker. Endocr. J. 2010, 57, 751–762. [Google Scholar] [CrossRef] [Green Version]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and Clinical Significance. JPEN J. Parenter. Enter. Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Kaysen, G.A. Biochemistry and biomarkers of inflamed patients: Why look, what to assess. Clin. J. Am. Soc. Nephro.l 2009, 4 (Suppl. 1), S56–S63. [Google Scholar] [CrossRef] [Green Version]
- Weaving, G.; Batstone, G.F.; Jones, R.G. Age and sex variation in serum albumin concentration: An observational study. Ann. Clin. Biochem. 2016, 53, 106–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gom, I.; Fukushima, H.; Shiraki, M.; Miwa, Y.; Ando, T.; Takai, K.; Moriwaki, H. Relationship between serum albumin level and aging in community-dwelling self-supported elderly population. J. Nutr. Sci. Vitaminol. 2007, 53, 37–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrillo, E.; Jimenez, M.A.; Sanchez, C.; Cunha, J.; Martins, C.M.; da Paixão Sevá, A.; Moreno, J. Protein malnutrition impairs the immune response and influences the severity of infection in a hamster model of chronic visceral leishmaniasis. PLoS ONE 2014, 9, e89412. [Google Scholar] [CrossRef] [PubMed]
- Hebeler, K.R.; Baumgarten, H.; Squiers, J.J.; Wooley, J.; Pollock, B.D.; Mahoney, C.; Filardo, G.; Lima, B.; DiMaio, J.M. Albumin is predictive of 1-year mortality after transcatheter aortic valve replacement. Ann. Thorac. Surg. 2018, 106, 1302–1307. [Google Scholar] [CrossRef] [Green Version]
- Hong, X.; Yan, J.; Xu, L.; Shen, S.; Zeng, X.; Chen, L. Relationship between nutritional status and frailty in hospitalized older patients. Clin. Interv. Aging 2019, 14, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.; Bochicchio, G.V.; Joshi, M.; Bochicchio, K.; Costas, A.; Tracy, K.; Scalea, T.M. Admission serum albumin is predicitve of outcome in critically ill trauma patients. Am. Surg. 2004, 70, 1099–1102. [Google Scholar]
- Yu, M.Y.; Lee, S.W.; Baek, S.H.; Na, K.Y.; Chae, D.W.; Chin, H.J.; Kim, S. Hypoalbuminemia at admission predicts the development of acute kidney injury in hospitalized patients: A retrospective cohort study. PLoS ONE 2017, 12, e0180750. [Google Scholar] [CrossRef] [Green Version]
- Lyons, O.; Whelan, B.; Bennett, K.; O’Riordan, D.; Silke, B. Serum albumin as an outcome predictor in hospital emergency medical admissions. Eur. J. Intern. Med. 2010, 21, 17–20. [Google Scholar] [CrossRef]
- Deniz, A.; Ozmen, C.; Bayram, E.; Seydaoglu, G.; Usual, A. Frailty significantly impairs the short term prognosis in elderly patients with heart failure. J. Geriatr. Cardiol. 2018, 15, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Boissonneault, A.R.; Schwartz, A.M.; Staley, C.A.; Schenker, M.L. Frailty and malnutrition are associated with inpatient postoperative complications and mortality in hip fracture patients. J. Orthop. Trauma. 2019, 33, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Dessì, M.; Noce, A.; Agnoli, A.; De Angelis, S.; Fuiano, L.; Tozzo, C.; Taccone-Gallucci, M.; Fuiano, G.; Federici, G. The usefulness of the prognostic inflammatory and nutritional index (PINI) in a haemodialysis population. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Mirili, C.; Yılmaz, A.; Demirkan, S.; Bilici, M.; Basol Tekin, S. Clinical significance of prognostic nutritional index (PNI) in malignant melanoma. Int. J. Clin. Oncol. 2019, 24, 1301–1310. [Google Scholar] [CrossRef] [PubMed]
- Garwe, T.; Albrecht, R.M.; Stoner, J.A.; Mitchell, S.; Motghare, P. Hypoalbuminemia at admission is associated with increased incidence of inhospital complications in geriatric trauma patients. Am. J. Surg. 2016, 212, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelman, D.T.; Adams, D.H.; Byrne, J.G.; Allred, E.N.; Cohn, L.H.; Rizzo, R.J. Impact of body mass index and albumin on morbidity and mortality after cardiac surgery. J. Thorac. Cardiovasc. Surg. 1999, 118, 866–873. [Google Scholar] [CrossRef] [Green Version]
- Akirov, A.; Masri-Iraqi, H.; Atamna, A.; Shimon, I. Low albumin levels are associated with mortality risk in hospitalized patients. Am. J. Med. 2017, 130, 1465.e11–1465.e19. [Google Scholar] [CrossRef] [Green Version]
- Salive, M.E.; Cornoni-Huntley, J.; Phillips, C.L.; Guralnik, J.M.; Cohen, H.J.; Ostfeld, A.M.; Wallace, R.B. Serum albumin in older persons: Relationship with age and health status. J. Clin. Epidemiol. 1992, 45, 213–221. [Google Scholar] [CrossRef]
- Tavani, C. A Staff Report. Public Policy and the Frail Elderly; DHEW Publication No. (OHDS) 79-20959; U.S. Department of Health, Education, and Welfare: Washington, DC, USA, 1978.
- Rockwood, K.; Hogan, D.B.; MacKnight, C. Conceptualisation and measurement of frailty in elderly people. Drugs Aging 2000, 17, 295–302. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, G.A. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Gobbens, R.J.J.; Luijkx, K.; Wijnen-Sponselee, M.; Schols, J.M.G.A. In search of an integral conceptual definition of frailty: Opinions of experts. JAMDA 2010, 11, 338–343. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Romano, L.; Marrone, G.; Noce, A.; Pujia, A.; Perrone, M.A.; Aiello, V.; Colica, C.; De Lorenzo, A. Role of personalized nutrition in chronic-degenerative diseases. Nutrients 2019, 11, 1707. [Google Scholar] [CrossRef] [Green Version]
- Soldati, L.; Di Renzo, L.; Jirillo, E.; Ascierto, P.A.; Marincola, F.M.; De Lorenzo, A. The influence of diet on anti-cancer immune responsiveness. J. Transl. Med. 2018, 16, 75. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Marchetti, M.; Cioccoloni, G.; Gratteri, S.; Capria, G.; Romano, L.; Soldati, L.; Mele, M.C.; Merra, G.; Cintoni, M.; et al. Role of phase angle in the evaluation of effect of an immuno-enhanced formula in post-surgical cancer patients: A randomized clinical trial. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1322–1334. [Google Scholar] [CrossRef] [PubMed]
- Plakht, Y.; Gilutz, H.; Shiyovich, A. Decreased admission serum albumin level is an independent predictor of long-term mortality in hospital survivors of acute myocardial infarction. Soroka Acute Myocardial Infarction II (SAMI-II) project. Int. J. Cardiol. 2016, 219, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.; Allard, J.; Vesnaver, E.; Laporte, M.; Gramlich, L.; Bernier, P.; Davidson, B.; Duerksen, D.; Jeejeebhoy, K.; Payette, H. Barriers to food intake in acute care hospitals: A report of the Canadian malnutrition task force. J. Hum. Nutr. Diet. 2015, 28, 546–557. [Google Scholar] [CrossRef]
- Naithani, S.; Thomas, J.E.; Whelan, K.; Morgan, M.; Gulliford, M.C. Experiences of food access in hospital. A new questionnaire measure. Clin. Nutr. 2009, 28, 625–630. [Google Scholar] [CrossRef]
- Arques, S.; Roux, E.; Sbragia, P.; Gelisse, R.; Pieri, B.; Ambrosi, P. Usefulness of serum albumin concentration for in-hospital risk stratification in frail, elderly patients with acute heart failure. Insights from a prospective, monocenter study. Int. J. Cardiol. 2008, 125, 265–267. [Google Scholar] [CrossRef]
- Menon, V.; Greene, T.; Wang, X.; Pereira, A.A.; Marcovina, S.M.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Sarnak, M.J. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Kidney Int. 2005, 68, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Chan, C.P.; Yan, B.P.; Zhang, Q.; Lam, Y.Y.; Li, R.J.; Sanderson, J.E.; Coats, A.J.; Sun, J.P.; Yip, G.W.; et al. Albumin levels predict survival in patients with heart failure and preserved ejection fraction. Eur. J. Heart Fail. 2012, 14, 39–44. [Google Scholar] [CrossRef]
- Phillips, A.; Shaper, A.G.; Whincup, P.H. Association between serum albumin and mortality from cardiovascular disease, cancer, and other causes. Lancet 1989, 2, 1434–1436, Erratum in: Lancet 1990, 335, 180. [Google Scholar] [CrossRef]
- Corti, M.C.; Guralnik, J.M.; Salive, M.E.; Sorkin, J.D. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994, 272, 1036–1042. [Google Scholar] [CrossRef]
- Rinninella, E.; Persiani, R.; D’Ugo, D.; Pennestrì, F.; Cicchetti, A.; di Brino, E.; Cintoni, M.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. NutriCatt protocol in the Enhanced Recovery After Surgery (ERAS) program for colorectal surgery: The nutritional support improves clinical and cost-effectiveness outcomes. Nutrition 2018, 50, 74–81. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency, N. (%) | Albumin Level, Mean (mg/dL) ± SD | p Values (ANOVA Test) | |
|---|---|---|---|---|
| Gender | Males | 5238 (55.6) | 3.392 ± 0.683 | NS |
| Females | 4190 (44.4) | 3.378 ± 0.614 | ||
| AGE (years) | <40 | 886 (9.4) | 3.734 ± 0.604 | All statistically significant p < 0.001 except 40–50 vs. 50–60 NS |
| 40-50 | 879 (9.3) | 3.558 ± 0.635 | ||
| 50-60 | 1502 (15.9) | 3.481 ± 0.641 | ||
| 60-70 | 2067 (21.9) | 3.393 ± 0.629 | ||
| 70-80 | 2340 (24.8) | 3.306 ± 0.584 | ||
| >80 | 1754 (18.6) | 3.143 ± 0.568 | ||
| CITIZENSHIP | Italian | 8674 (92) | 3.376 ± 0.630 | |
| Foreign | 754 (8) | 3.501 ± 0.652 | <0.001 | |
| MARITAL STATUS | Single | 1638 (17.4) | 3.494 ± 0.650 | Single vs. Married |
| Married | 7245 (76.8) | 3.360 ± 0.628 | <0.001 | |
| Separated/Divorced | 218 (2.3) | 3.420 ± 0.638 | ||
| Widow | 327 (3.5) | 3.382 ± 0.597 | Single vs. Widow = 0.035 | |
| EDUCATION | Illiterate | 83 (0.9) | 3.385 ± 0.593 | Prim. vs. Int. <0.001 |
| Primary School | 1242 (13.2) | 3.270 ± 0.592 | Prim. vs. Sec. <0.001 | |
| Intermediate School | 6211 (65.9) | 3.357 ± 0.626 | Prim. vs. High <0.001 | |
| Secondary School | 1570 (16.7) | 3.551 ± 0.654 | Int. vs. Sec. <0.001 | |
| Higher Education | 322 (3.4) | 3.578 ± 0.630 | Int. vs. High = 0.044 |
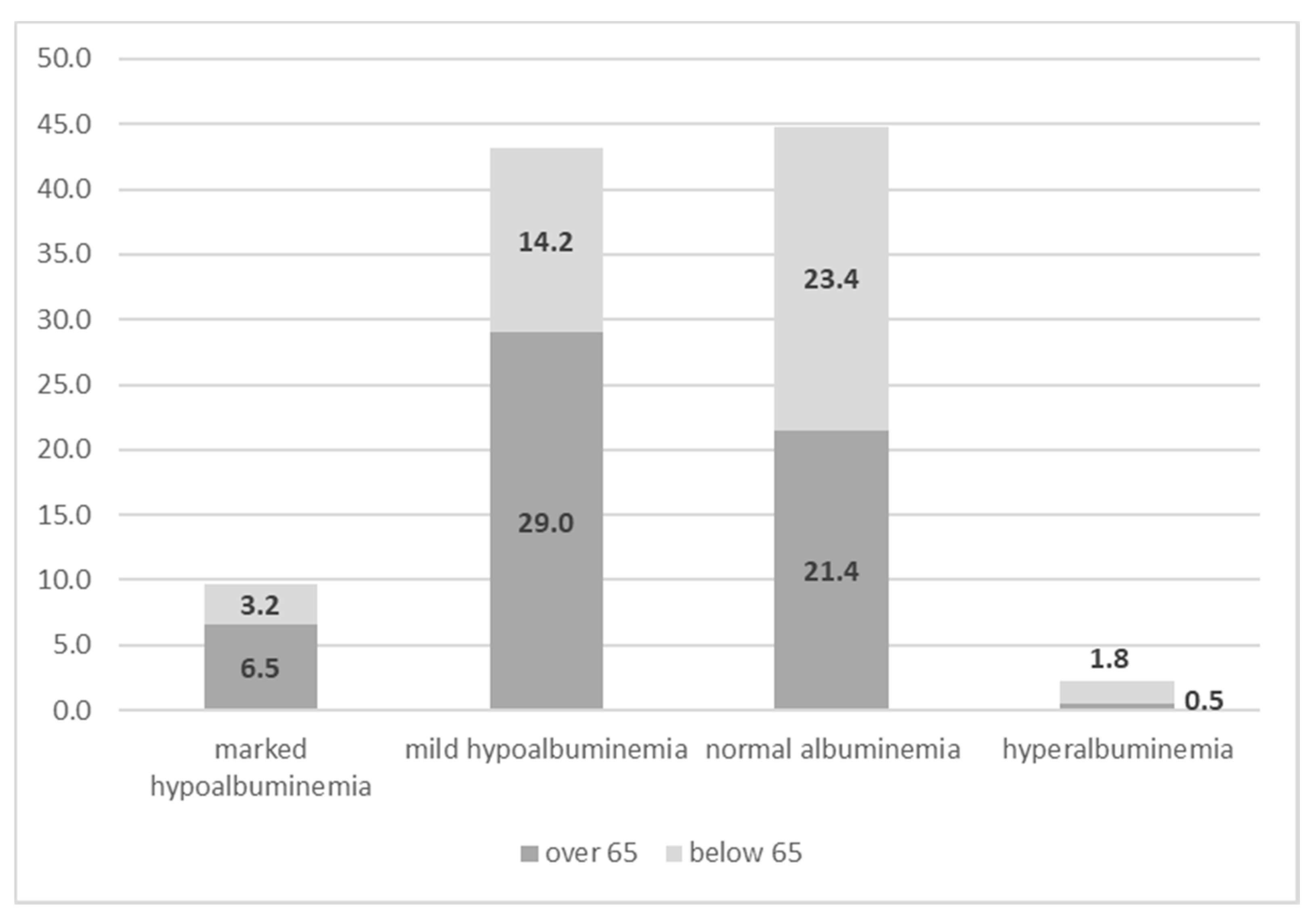
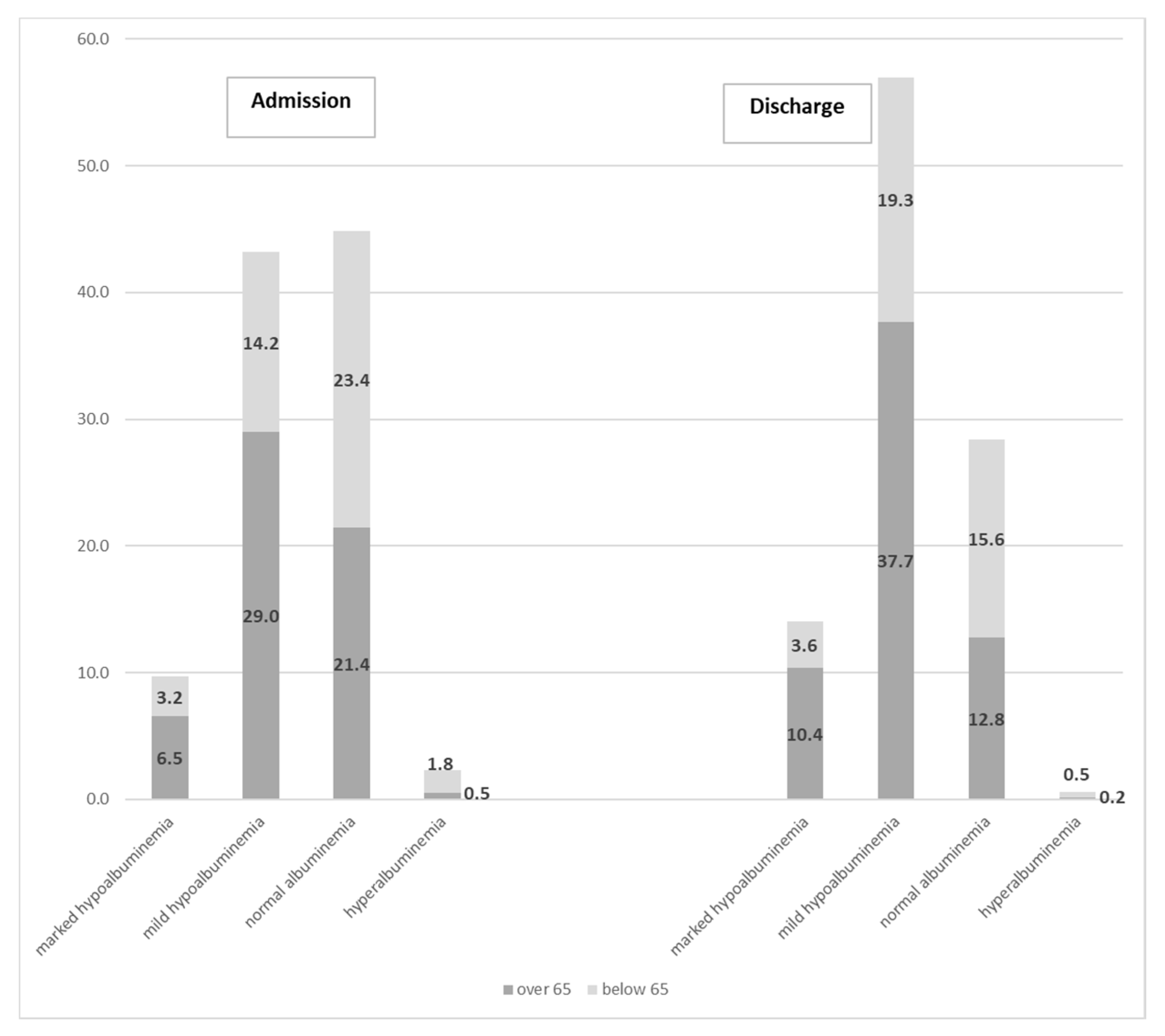
| Albuminemia at Baseline | Frequency n, (%) | Value, Mean Value ± SD | Prevalence in >65 Years Old, n, (%) | Prevalence in <65 Years Old, n, (%) |
|---|---|---|---|---|
| Marked hypoalbuminemia (<2.5 mg/dL), and | 909 (9.6) | 2.177 ± 0.288 | 613 (67.4) | 296 (32.6) |
| p < 0.001 | ||||
| Mild hypoalbuminemia (2.5–3.5 mg/dL) | 4045 (42.9) | 3.073 ± 0.267 | 2714 (67.1) | 1331 (32.9) |
| p < 0.001 | ||||
| Normal albuminemia (3.5–4.5 mg/dL) | 4199 (44.5) | 3.884 ± 0.259 | 2009 (47.8) | 2190 (52.2) |
| p < 0.001 | ||||
| Hyperalbuminemia (>4.5 mg/dL) | 214 (2.3) | 4.645 ± 0.127 | 46 (21.5) | 168 (78.5) |
| p < 0.001 | ||||
| Major Diagnostic Categories (MDC24) | Frequency | Percentage | Albumin at Baseline (mg/dL), Mean ± SD |
|---|---|---|---|
| diseases and disorders of the nervous system (1) | 1830 | 19.8 | 3.663 ± 0.481 |
| diseases and disorders of the respiratory system (4) | 1299 | 14.1 | 3.254 ± 0.621 |
| diseases and disorders of the circulatory system (5) | 1194 | 12.9 | 3.134 ± 0.621 |
| diseases and disorders of the musculoskeletal system and connective tissue (8) | 1128 | 12.2 | 3.471 ± 0.535 |
| diseases and disorders of the digestive system (6) | 945 | 10.2 | 3.324 ± 0.667 |
| diseases and disorders of the hepatobiliary system and pancreas (7) | 831 | 9.0 | 3.291 ± 0.651 |
| myeloproliferative DDs (poorly differentiated neoplasms) (17) | 429 | 4.6 | 3.485 ± 0.616 |
| diseases and disorders of the kidney and urinary tract (11) | 404 | 4.4 | 3.297 ± 0.692 |
| infectious and parasitic DDs (Systemic or unspecified sites) (18) | 178 | 1.9 | 2.861 ± 0.591 |
| factors influencing health status and other contacts with health services (23) | 177 | 1.9 | 3.578 ± 0.674 |
| diseases and disorders of the endocrine, nutritional and metabolic system (10) | 169 | 1.8 | 3.472 ± 0.578 |
| diseases and disorders of the blood and blood forming organs and immunological disorders (16) | 144 | 1.6 | 3.372 ± 0.646 |
| diseases and disorders of the skin, subcutaneous tissue and breast (9) | 102 | 1.1 | 3.328 ± 0.645 |
| diseases and disorders of the ear, nose, mouth and throat (3) | 96 | 1.0 | 3.897 ± 0.56 |
| mental diseases and disorders (19) | 95 | 1.0 | 3.552 ± 0.531 |
| injuries, poison and toxic effect of drugs (21) | 70 | 0.8 | 3.014 ± 0.761 |
| diseases and disorders of the eye (2) | 51 | 0.6 | 3.991 ± 0.402 |
| multiple significant trauma (24) | 46 | 0.5 | 3.027 ± 0.689 |
| human Immunodeficiency virus infection (25) | 21 | 0.2 | 3.235 ±0.845 |
| diseases and disorders of the male reproductive system (12) | 13 | 0.1 | 3.243 ± 0.669 |
| diseases and disorders of the female reproductive system (13) | 13 | 0.1 | 3.328 ± 0.507 |
| alcohol/drug use or induced mental disorders (20) | 6 | 0.1 | 3.418 ± 0.623 |
| newborn and other neonates (perinatal period) (15) | 3 | 0 | 3.483 ± 0.317 |
| burns (22) | 1 | 0 | 3.030 |
| Total | 9245 | 100 | 3.385 ± 0.629 |
| MDC24 | Diagnosis of Hospitalization (DRG24) | Frequencies | Percentages | Albumin at Baseline (Mg/Dl), Mean ± SD | Significant Differences among Drgs: p Values <0.05 (ANOVA Test) |
|---|---|---|---|---|---|
| 1 | Transient cerebral ischemia (524) | 101 | 1.1 | 3.670 ± 0.442 | vs. 87, 89, 104, 127, 179, 202, 210, 544, 569 |
| 17 | Acute leukemia without major surgery (473) | 101 | 1.1 | 3.570 ± 0.547 | vs. 87, 89, 104, 127, 179, 202, 210, 569 |
| 6 | Inflammatory diseases of intestine (179) | 102 | 1.1 | 3.300 ± 0.584 | vs. 2, 12, 14, 75, 104, 219, 467, 473, 543 |
| 6 | Major surgery of both large and small intestine (569) | 104 | 1.1 | 3.285 ± 0.826 | vs. 2, 12, 14, 75, 219, 410, 467, 473, 524, 543, 544 |
| 23 | Other factors affecting the state of health (467) | 110 | 1.2 | 3.900 ± 0.624 | vs. 87, 89, 104, 127, 179, 202, 210, 410, 544, 569 |
| 8 | Operation on the lower limb and humerus except hip. foot and femur (219) | 124 | 1.3 | 3.600 ± 0.418 | vs. 87, 89, 104, 127, 179, 202, 210, 544, 569 |
| 17 | Chemotherapy not associated with secondary diagnosis of acute leukemia (410) | 127 | 1.3 | 3.440 ±0.545 | vs. 2, 12, 75, 87, 89, 104, 202, 210, 467, 569 |
| 1 | Degenerative diseases of the nervous system (12) | 136 | 1.4 | 3.830 ± 0.436 | vs. 87, 89, 104, 127, 179, 202, 210, 410, 544, 569 |
| 1 | Craniotomy with major device implant or major diagnosis of complex acute pathology of the central nervous system (543) | 143 | 1.5 | 3.570 ± 0.426 | vs. 87, 89, 104, 127, 179, 202, 210, 569 |
| 8 | Hip and femur surgery. except major joints (210) | 147 | 1.6 | 3.090 ± 0.420 | vs. 2, 12, 14, 75, 219, 410, 467, 473, 524, 543, 544 |
| 5 | Heart valve surgery and other major cardiothoracic surgeries with cardiac catheterization (104) | 155 | 1.6 | 2.800 ± 0.562 | vs. 2, 12, 14, 75, 87, 127, 179, 202, 410, 467, 473, 524, 543, 544 |
| 1 | Craniotomy (2) | 165 | 1.8 | 3.800 ± 0.408 | vs. 87, 89, 104, 127, 179, 202, 210, 410, 544, 569 |
| 7 | Cirrhosis and alcoholic hepatitis (202) | 177 | 1.9 | 3.040 ± 0.665 | vs. 2, 12, 14, 75, 104, 219, 410, 467, 473, 524, 543, 544 |
| 5 | Heart failure and shock (127) | 179 | 1.9 | 3.300 ± 0.516 | vs. 2, 12, 14, 75, 87, 104, 219, 467, 473, 524, 543 |
| 4 | Major interventions on the chest (75) | 180 | 1.9 | 3.770 ± 0.540 | vs. 87, 89, 104, 127, 179, 202, 210, 410, 544, 569 |
| 4 | Pulmonary edema and respiratory failure (87) | 204 | 2.2 | 3.090 ± 0.598 | vs. 2, 12, 14, 75, 104, 127, 219, 410, 463, 473, 524, 543, 544 |
| 8 | Replacement of major joints or reimplantation of the lower limbs (544) | 305 | 3.2 | 3.395 ± 0.449 | vs. 2, 12, 14, 75, 87, 89, 104, 202, 210, 219, 467, 524, 569 |
| 4 | Simple pneumonia and pleurisy (89) | 325 | 3.4 | 3.100 ± 0.569 | vs. 2, 12, 14, 75, 127, 219, 410, 467, 473, 524, 543, 544 |
| 1 | Intracranial hemorrhage or cerebral infarction (14) | 551 | 5.8 | 3.700 ± 0.469 | vs. 87, 89, 104, 127, 179, 202, 210, 544, 569 |
| Totals | 3,436 | 36.4 | 3.403 ± 0.595 |
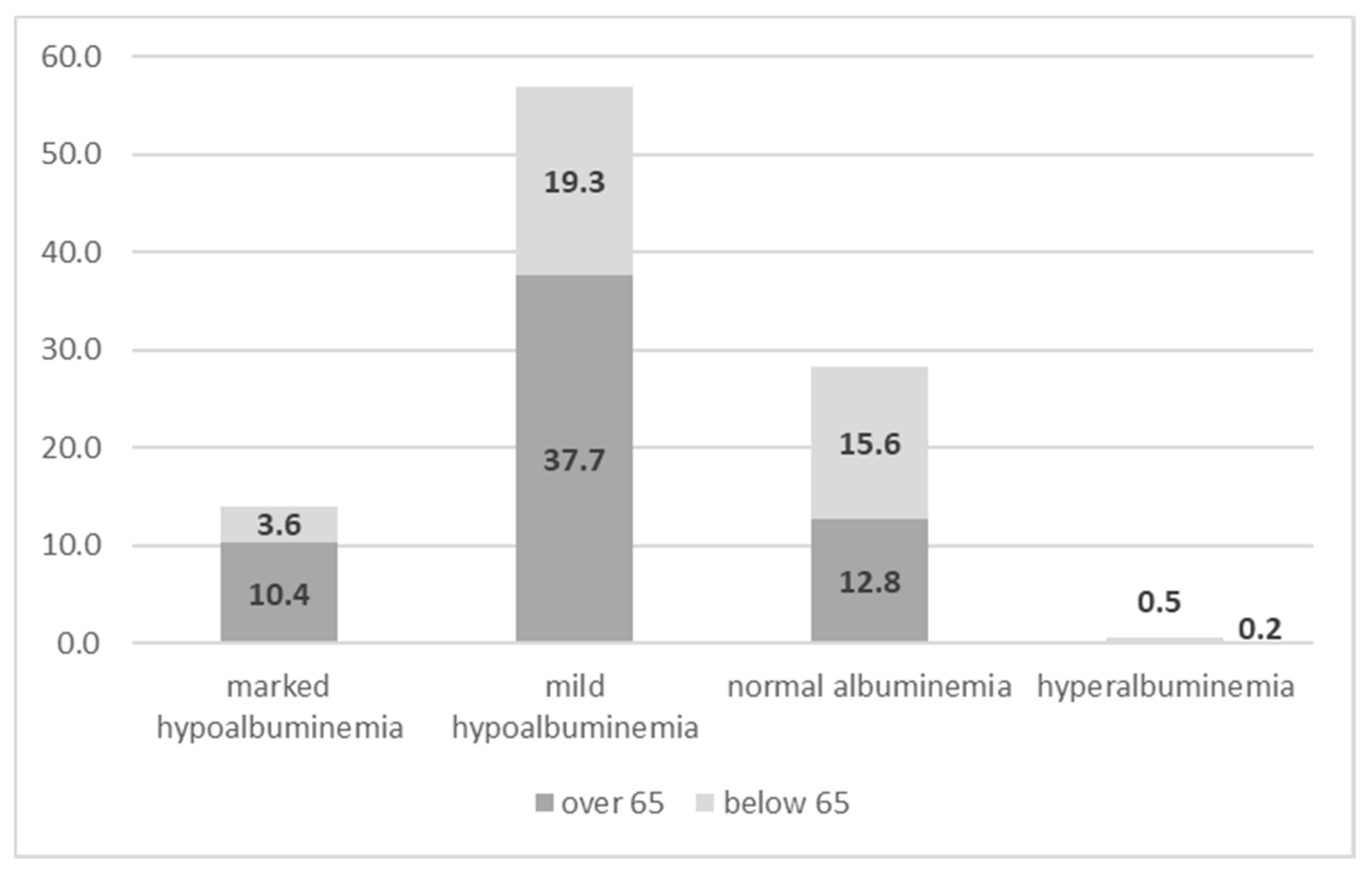
| Albuminemia at Second Dosage | Frequency n, (%) | Value, Mean Value ± SD | Prevalence in Patients over 65 Years Old, n, (%) | Prevalence in Patients below 65 Years Old, n, (%) |
|---|---|---|---|---|
| Marked hypoalbuminemia (<2.5 mg/dL), and | 912 (14) | 2.156 ± 0.277 | 677 (74.2) | 235 (25.8) |
| p < 0.001 | ||||
| Mild hypoalbuminemia (2.5–3.5 mg/dL) | 3709 (57) | 3.019 ± 0.281 | 2452 (66.1) | 1257 (33.9) |
| p < 0.001 | ||||
| Normal albuminemia (3.5–4.5 mg/dL) | 1847 (28.4) | 3.808 ± 0.238 | 830 (44.9) | 1017 (55.1) |
| p < 0.001 | ||||
| Hyperalbuminemia (>4.5 mg/dL) | 40 (0.6) | 4.678 ± 0.142 | 10 (25) | 30 (75) |
| p < 0.001 | ||||
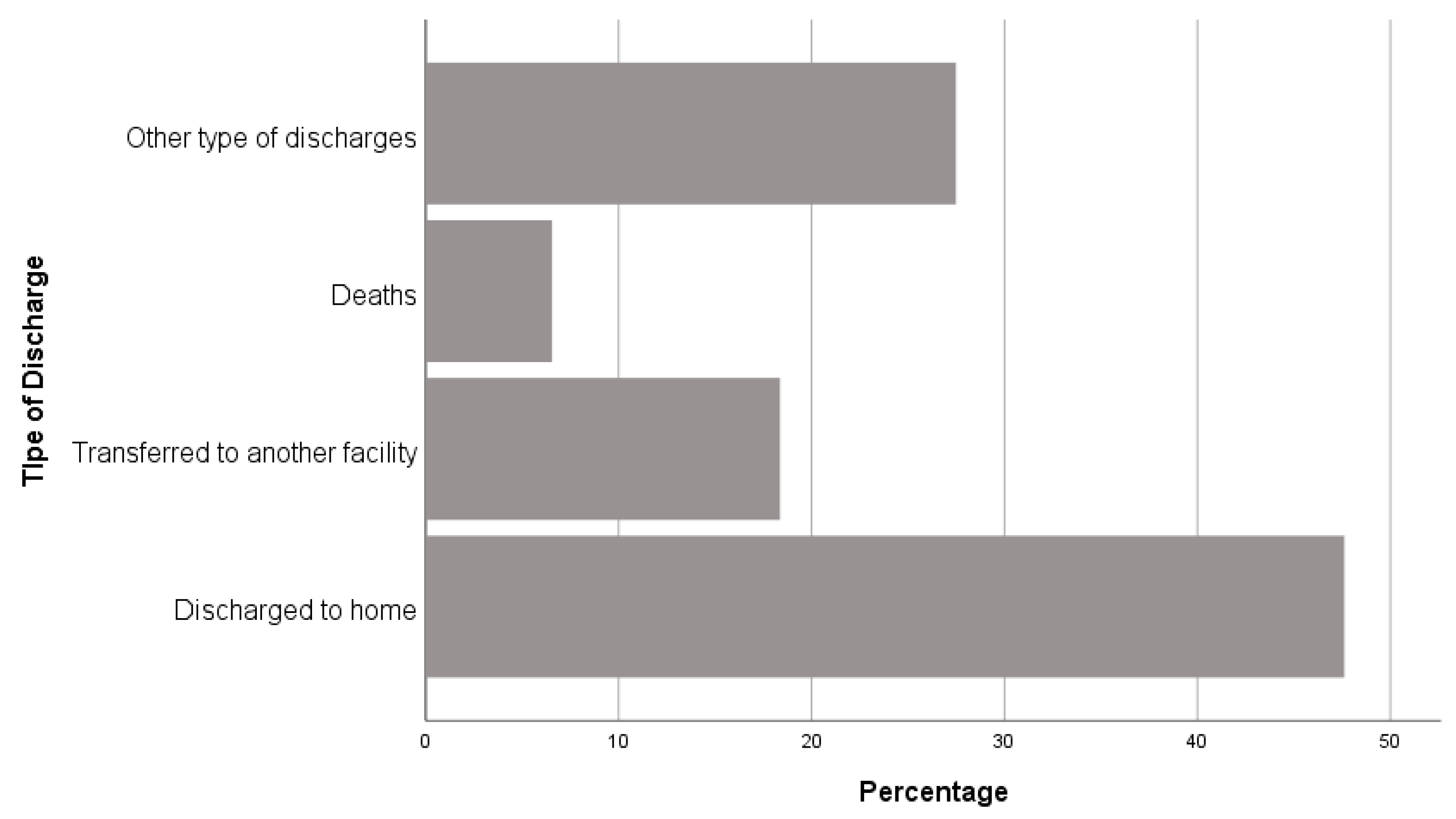
| Outcome | Albumin Level, Mean (mg/dL) ± SD | p Value (ANOVA Test) |
|---|---|---|
| discharged home | 3.455 ± 0.610 | Death vs. all <0.001 Transferred vs. all <0.001 Discharged to home vs. other type of discharge NS |
| transferred to long-term health care facilities | 3.222 ± 0.598 | |
| death | 2.839 ± 0.669 | |
| other type of discharge | 3.504 ± 0.597 |
| Outcome | Variable | Exp(B) | Significance | 95% CI Per Exp(B) |
|---|---|---|---|---|
| Death | Divorced | 2.745 | 0.029 | 1.110–6.786 |
| Widow | 2.561 | 0.004 | 1.340–4.893 | |
| Sex (male vs. female) | 1.376 | <0.001 | 1.153–1.641 | |
| Age | 1.029 | <0.001 | 1.023–1.036 | |
| Albumin at admission | 0.270 | <0.001 | 0.236–0.310 | |
| Discharged home | Single | 0.811 | <0.001 | 0.724–0.997 |
| Higher education | 0.765 | 0.020 | 0.609–0.959 | |
| Age | 0.995 | <0.001 | 0.992–0.997 | |
| Albumin at admission | 1.328 | <0.001 | 1.241–1.421 | |
| Transferred to long-term health care facilities | Single | 1.213 | 0.019 | 1.033–1.424 |
| Secondary | 1.637 | <0.001 | 1.358–1.973 | |
| Higher | 1.798 | 0.002 | 1.237–2.613 | |
| Sex (male vs. female) | 0.821 | <0.001 | 0.738–0.914 | |
| Age | 1.018 | <0.001 | 1.014–1.022 | |
| Albumin at admission | 0.699 | <0.001 | 0.641–0.762 | |
| Other types | Single | 1.283 | <0.001 | 1.127–1.461 |
| Secondary | 0.825 | 0.003 | 0.728–0.935 | |
| Age | 0.989 | <0.001 | 0.986–0.992 | |
| Albumin at admission | 1.399 | <0.001 | 1.295–1.512 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moramarco, S.; Morciano, L.; Morucci, L.; Messinese, M.; Gualtieri, P.; Carestia, M.; Ciccacci, F.; Orlando, S.; Buonomo, E.; Legramante, J.M.; et al. Epidemiology of Hypoalbuminemia in Hospitalized Patients: A Clinical Matter or an Emerging Public Health Problem? Nutrients 2020, 12, 3656. https://doi.org/10.3390/nu12123656
Moramarco S, Morciano L, Morucci L, Messinese M, Gualtieri P, Carestia M, Ciccacci F, Orlando S, Buonomo E, Legramante JM, et al. Epidemiology of Hypoalbuminemia in Hospitalized Patients: A Clinical Matter or an Emerging Public Health Problem? Nutrients. 2020; 12(12):3656. https://doi.org/10.3390/nu12123656
Chicago/Turabian StyleMoramarco, Stefania, Laura Morciano, Luca Morucci, Mario Messinese, Paola Gualtieri, Mariachiara Carestia, Fausto Ciccacci, Stefano Orlando, Ersilia Buonomo, Jacopo Maria Legramante, and et al. 2020. "Epidemiology of Hypoalbuminemia in Hospitalized Patients: A Clinical Matter or an Emerging Public Health Problem?" Nutrients 12, no. 12: 3656. https://doi.org/10.3390/nu12123656